{kind=link}
Gluco-Beta Stimulator
Posted by Nutrition Works on
Gluco-Beta-Stimulator
"Assists in the control of diabetes and its associated physiological symptoms and conditions; potentially reduces blood sugar, regeneration/ repair of the pancreatic beta cells in the islets of Langerhans."
I. Introduction
Both traditional and natural healthcare providers have a responsibility to assist in care of the epidemic of diabetes mellitus. The World Health Organization estimated that the number of diabetics has increased from 200 million worldwide, in the year 2000, to 346 million in 2011.1Whether one is an allopathic or natural care practitioner, diabetes needs to be confronted. It is uncommon to review a patient history without coming across diabetes or its associated diseases/complications within the patient history, family unit, or family tree.
Diabetes is a chronic metabolic disorder that disrupts the biochemical pathways involving carbohydrate, fat, and protein metabolism. There are three types of diabetes. Type one is characterized as insulin dependent diabetes. The hormone insulin regulates the glucose in the bloodstream. In Type one diabetes, the beta cells, which are responsible for the secretion of insulin, of the pancreas are completely destroyed. Type two diabetes effects 90% of all diagnosed persons with diabetes and is also characterized as non-insulin dependent diabetes.2 This hyperglycemia involves an impairment of insulin effectiveness, or insulin resistance. The third type of diabetes occurs when the pancreas is over working during a pregnancy; this occurs in fourteen percent of all pregnant women.3 Although the condition reverses upon delivery, women diagnosed with type three diabetes are 9.6 times as likely to develop type two diabetes after age 40.
II. Causations
The amount of people that are impacted by insulin dependent diabetes is on the rise. Traditionally, insulin dependent diabetes only affected children; however destruction of the pancreatic beta cells is occurring in adults now as well. Viral infections such as mumps, hepatitis, rubella, and other childhood diseases can destroy the beta cells.2 This destruction may, in turn, ultimately lead to type one diabetes. Historically this type of diabetes was called juvenile diabetes because only early childhood diseases would lead to the complete destruction of theses insulin producing cells. However, in recent years it has been demonstrated that some prescription drugs, such as Streptosotocin,2 statins,4 antidepressants,5 glucocorticoid steroids,6 and antipsychotics also destroy the beta cells.7 Researchers concluded that patients taking selective serotonin re-uptake inhibitors and tricyclic antidepressants for a year or more were at an increased risk for developing diabetes.5 Such pharmaceuticals cause significant weight gain and impairment of the glucose homeostasis.5 In a recent study, it was concluded that "glucocorticoid cause insulin resistance by inhibiting glucose uptake and reducing glucose storage.”6 This study also confirmed that steroid use, i.e. prednisone, for over a year, leads to the destruction of beta cells.6 In addition, studies have shown that corticosteroid treatment also increases the urinary secretion of chromium.8 An increased deficiency of chromium also contributes to the diabetic syndrome. Such steroids also include any dermal steroid creams used to treat skin infections or poison as well as steroids for eyes or nose.
Type two diabetes, or non-insulin dependent diabetes, was most prevalent among the adult populations ranging from ages 50-70 years.9 As the body ages, the beta cells of the pancreas become strained. The beta cells produce insulin, however, the body fails to respond to the hormone causing an insulin resistance. Typically, a diet rich in refined sugars causes the beta cells to become strained, rendering them ineffective and causing insulin resistance syndrome As a result of its attempt to rid the body of the excessive sugar in the blood, the pancreas over works itself .10 An error in the target tissues for glucose, the liver, muscle, or adipose tissue is also possible.10 The pancreas, consequently, will compensate by making more insulin, however, the body's cells resist the hormone causing glucose to accumulate in the blood. It is common, as a result, to find such patients making over 300 times the amount of glucose necessary suggesting an error in metabolism.
Unfortunately, there has been a dynamic shift in the age group of diagnosis. America is seeing a large number of children with type two diabetes due to the "western diet" filled with excessive refined sugars.10 Younger adults ranging from 30-60 years old are being diagnosed with type one diabetes. Such diagnosises are apparent because it has been shown that diabetics have 63% less beta cell mass.11 This younger population seems to have a suppression of insulin levels leading to the belief that the beta cell number is decreasing because of the destruction of the beta cells due to pharmaceuticals.
CHART 1
Chart of Associated Conditions
|
Heart Disease |
Stroke |
Hypertension |
|
Hyperlipidemia |
Kidney Disease |
Blindness |
|
Nervous System Diseases |
Neuropathies |
Gastroparesis |
|
Peripheral Arterial Disease |
Ketoacidosis |
Hyperosmolar Hyperglycemic non-ketotic Syndrome |
|
Skin Conditions |
Blood Clots |
Cellulititis |
|
Xerostomia |
Liver Diseases |
Impotence |
|
High Cholesterol |
Steatosis |
Optic Neuritis |
|
Overactive Bladder |
Restless Leg Syndrome |
Fatigue |
|
Foot Problems |
Dental Diseases |
Obesity |
The associated conditions set out in Chart 1 relate to the impact of hyperglycemia on the whole body systems. Increased blood glucose levels lead to an inflammation of the microcirculation of the kidneys, nerves, lens, pancreas, and blood vessels of the heart.12 This inflammation is due the increase in the glycation end products because of the chronic elevated sugar levels in the blood. Diabetics statistically have a "two-to fourfold greater risk of cardiovascular disease, a fivefold increased risk of blindness and four times the rate of kidney disease reports Andus and colleagues.13
III. Diagnostic
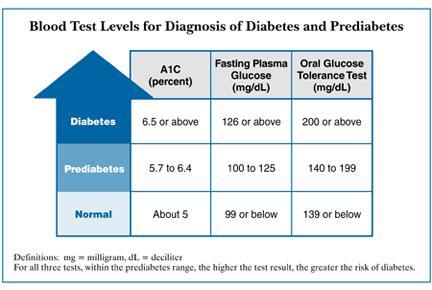
The Oral Glucose Tolerance Test (“GTT”) is typically used in the diagnosis of diabetes. This test is extremely stressful to the patient. The standard of fasting blood glucose is 70 - 105 mg/dL; above 140mg/dL on two occasions is considered a diagnostic diabetes.2 The GTT tests the blood glucose levels of the patient after administrating 75grams of glucose in 300mL of water. There is a positive diagnosis of diabetes if the patient exhibits plasma glucose above 200 mg/dL at the two-hour and four-hour measurement.2
Another test, called the hemoglobin A1C, measures the level of glycosylated hemoglobin. This diabetic marker is a one-time stick blood test that will predict a risk level or the severity of this disease. An A1C is a blood test that shows up to a three-month pattern of the health of the pancreas including an average blood glucose level. There is an increase in the percentage of hemoglobin bound to glucose when there is excessive sugar in the blood. The normal concentration is 5-7%.2
Clinically, we began to observe trends in blood sugars over 20 years ago. More recently, we have been evaluating our patient's hemoglobin A1C. The longer hyperglycemia occurs in blood, the more glucose binds to red blood cells and the higher the glycosylated hemoglobin. According to the American Diabetes Association (“ADA”), a diagnosis of diabetes is concurrent with an A1C at 7 or above.14 However, most laboratories rate the A1C at below 5.6 as normal, 5.7-5.8 equates to pre-diabetic, and 6 or above equates to a diagnosis of diabetes. We are seeing a precedent of symptoms including disruptions in the microcirculation of the tiny blood vessels of the feet, eyes, heart, and nephron units before the A1C diagnoses diabetes. The symptoms beg the question: if we regularly screen those patients with familiar risk or onset of suspicious symptom is there a way to interrupt the progression of the disease and the associated diseases naturally?
CHART 2
IV. Allopathic Approach
Traditionally, diabetes has been treated with injectable insulin or oral agents. Insulin injections are most common among type one. Side effects of insulin injections for type one diabetics include swelling, itching, rashes, fast heartbeats, low blood pressure, and interactions with aspirin and foods.16 A synthetic form of amylin, Pramlintide is used along with insulin and glucagon to also maintain blood glucose levels. Another injectable agent, Exenatide, works to lower glucose levels by increasing insulin secretion. Pharmaceuticals include a class of oral medications that are used to stimulate the beta cells to release more insulin such as Sulfonylureas, Meglitinides and Chlorpropanimide. In addition, there are medications that block the breakdown of starches; these include Alpha-glucosides inhibitors and DPP-4 inhibitors. Finally, the most widely used medication for diabetes is Metformin. First synthesized in 1922 and observed in a clinical trial in 1957, Metformin improves the hyperglycemia by suppressing glucose production and conversion in the liver or gluconeogenesis.17 Some of the side effects of Metformin include bloating, diarrhea, nausea, upset stomach, lactic acidosis, and a metallic taste in the mouth.16 Other complications that follow Metformin are an overall increased risk of heart disease related deaths.18 It is clear that over the years allopathic medicine has made headway in controlling the diabetics and vigorously trying to make an impact on the associated conditions. However, there is no repair mechanism in the error of metabolism that is causing this disease. Rather, these drugs can only balance the blood sugar circulating in the body; therefore the patients are on these prescription medications for the remainder of their lives.16
It is also worthy to note that such anti-diabetic pharmaceuticals are a burden to the health care system. In 2002, it was reported that an estimated $132 billion was distributed to diabetes and $92 billion of that was direct medical costs.19
V. Dietary Interventions
Dietary intervention is helpful in assisting in the care of a diabetic individual. It is known that Americans consume an average of 149.2 pounds of refined sugar in a year's time.19 This equates to approximately three pounds per week and 41 teaspoons per day. This massive amount of refined sugar and refined flours causes an increased level of triglycerides which increases the resistance to insulin. Type two diabetes can be controlled with a drastic diet intervention. Unfortunately, patient compliance is heavily weighed on such drastic intervention, thus physicians cannot rely on such treatment. The benefits of high complex carbohydrate, high fiber diet on the glycemic index versus a low carbohydrate, high protein diet is heavily disputed.20 Some research supports a low-protein, low fat, high carbohydrate diet due to the stress that protein places on the kidneys. It is also thought that increased carbohydrates lead to increased secretion of insulin.10 Therefore, after much research the ADA now advocates an individualized diet with proportional amounts of protein, carbohydrates, and fat.
The glycemic index (“GI”) measured how much food affects a person’s blood sugar and how fast the food is digested into glucose.10 The higher the GI the greater the rise in blood sugar after consumption. Many dietitians suggest that a low glycemic load and increased physical activity will stimulate glycogen synthesis and improve beta cells activity. 13
VI. Nutrition Interventions by a Complementary Care Medical Provider
Initially, natural healthcare providers sought a product, to treat diabetes, that would intervene in the metabolic imbalance of diabetes with the hope that such a product would decrease the need for pharmaceuticals, as well as combat the associated conditions that follow a lack of blood sugar control. To that end, we began to utilize chromium, biotin, cinnamon, and Gymnema sylvestre as individual products.
It is common to find a chromium deficiency among patients with type one and type two diabetes as well as gestational diabetes.20 Chromium deficiency leads to impaired metabolism and nerve function.8 Chromium also facilitates the cellular uptake of glucose by working with insulin,2 without this cofactor, the action of insulin is inhibited and glucose and insulin accumulate in the body systems. In addition, Chromium decreases blood lipid values such as cholesterol and triglycerides.10
Biotin is a water-soluble B vitamin that is involved in the metabolism of carbohydrates and lipids. This vitamin enhances the effects of chromium and increases the beta cell expression of the enzyme glucokinase, which is involved for the conversion of glucose to ATP.22 This ATP fuels the mechanisms needed to regulate blood glucose. In a study that evaluated the effects of 600 ug of chromium with 2mg of biotin on patients with an A1C greater than 7, at the end of the 90 day randomized, double blind trial, the mean A1C decreased by 0.54% in the study group. The mean fasting glucose also decreased by 9.8mg/dL in the study group.21
Cinnamon as Cinnamomum cassia is thought to have insulin stimulating properties due to it capabilities to enhance the insulin receptor autophosphorylation. This activation of the receptor increases insulin sensitivity.19 By stimulating the receptor for insulin, cinnamomum cassia enhances regulation of sugar that is extracted from the carbohydrates.16 In a study conducted by Khan et al. in 2003 the effects of cinnamon were evaluated on 60 type two diabetics on sulfonyurea medications. The trial measured the fasting serum glucose levels. At the end of this study it was apparent that administration of 1-6 grams of cinnamon per day decreased the fasting serum glucose levels (p<0.05).19 To the contrary, The placebo group’s glucose levels rose from 0.6% to 2.7%. The test group demonstrated other improvements including a decrease in cholesterol and triglyceride levels.19
The Indian herb, Gymnema sylvestre, was traditionally used to suppress the sweet taste of sugar. For over 2,000 years, in Ayurverdic medicine in India, Gymnema was traditionally used for glycosuria, urinary disorders, and diabetes mellitus.23 The common name, "gurmar" translates to "sugar destroyer."24 Gymnema also contain gymnemosides and amino acids that are known to stimulate beta-cell function and glucose uptake and utilization.21 In a research model this herb was found to increase the activity of the glucose utilization enzymes.12 Suggested mechanisms of Gymnema are thought to be its ability to inhibit intestinal absorption of glucose and increase the activity of the enzymes used in blood glucose regulation pathways.23 The active "parts" of the Indian plant include a peptide gumarin, anti-sweet saponins, stigmasterol, quercitol, gymnemic acids, and amino acid derivatives betaine, choline, and trimethylamine. With these components, Gymnema sylvestre has been shown to reduce blood glucose, glycosylated hemoglobin, and glycosylated plasma proteins.24 The increase in insulin levels after supplementation support the claim that Gymnema repairs and rejuvenates the pancreatic beta cells.23
In a study, evaluating the effectiveness of 400mg/day of G. sylvestre it was reported that there was a significant reduction in the fasting blood glucose levels and the insulin requirements in patients with insulin-dependent diabetes.12 An extract of this herb doubled the number islet and beta cells in the pancreas in one study conducted by Prakash.20 Other studies reported an improvement of glycolysis, gluconeogenesis, muscle glucose uptake, and a decrease in protein glycosylation.13 Though various studies, it is confirmed that Gymnema rejuvenated the pancreas and reverses the damage to the beta cells.16
In a placebo controlled randomized study, researchers reported lower glucose/insulin ratio after supplementation thus concluding a decrease in insulin resistance.24 This decrease in insulin resistance was also assessed by an increase in beta cell function. In this study, diabetic patients also had reduced symptoms such as suppressed hunger and decreased fatigue. Overall, there was a reduction in hyperglycemia which reduces the metabolic risk of the development of secondary complications of diabetics.24
In a controlled, nonrandomized, nonblinded study of 47 patients with type two diabetes documented in 1990, 400mg of Gymnema sylvestre was given to 22 patients for 18-20 months. Fasting glucose levels were 29% (p<0.001) lower than baseline and the hemoglobin A1C deceased from baseline on average 11.91%-8.48% (p<0.001). Additionally five patients were able to discontinue the hypoglycemic medications.25 There were no significant changes in the oral hypoglycemic medications group. This plant has also demonstrated implications on weight loss,26 hyperlipidemia,23 and decrease in fatigue.24
The combination of chromium, biotin, cinnamon, and Gymnema sylvestre is most effective in lowering glucose levels and AlC across the board. Independent nutrients were used synergistically for over five years in our practice. By continuously recording their blood sugar and routine A1C we were able to see between 85-95% of our clients improve. They had regression of metabolic syndromes associated with diabetes such as less pain in their feet, kidney function improvement, and improvement of neuropathies associated with the eyes.
Unfortunately, about 5-10% did not respond due to non-compliance with the amount of products in this regimen. At our request Professional Health Products (PHP) became involved in the production of Gluco-Beta-Stimulator (GBS) in order to combine chromium, biotin, cinnamon, and Gymnema sylvestre into one capsule. Within the last three years, we have noticed considerable improvement in the hemoglobin A1C by adding GBS to our client supplement regiment. This is very possible due to the availability a capsule with each of the four supplements instead of a combination of supplements; this lesser amount of supplements also aids in client compliance.
Currently, we are undergoing a study in our practice to evaluate the change in hemoglobin A1C and the fasting blood sugars after administration of four Gluco-Beta-Stimulators a day for one year. Our study has approximately forty clients and we are monitoring their blood sugar every two to three months and their hemoglobin A1C every four to six months. However, we are continuously adding new clients to our study each week. Our preliminary data has shown great efficacy in the administration of GBS. In citing a few of our case studies, a 66 year old female patient had a hemoglobin A1C of 6.5 in June 2012 and a random glucose of 140mg/dL, within six months on GBS her A1C was reduced to 6.0 and her random glucose was 120 mg/dl. (CS#16). Another, patient was straddling the line of pre-diabetes and diabetic associated symptoms for a number of years. In October of 2012, his hemoglobin A1C was 12.7 and a random glucose of 305mg/dL. (CS#18). His doctor wanted to place him on insulin therapy right away, but he refused. Turning to our care, we advised him to cut back his consumption of sweets and desserts and implement our GBS regimen of four capsules per day. Within three months his A1C went down to 7.3 and his random glucose was 128mg/dL. Within the year we expect that his A1C will be below the diabetic threshold.
Improvements in some of the associated diseases of diabetes have been noticed with this product. In one case, a patient with a short term diagnosis of kidney failure came into our practice. Her kidney function went up and down while being treated with the suggested kidney support nutrients. We suggested an evaluation of A1C to determine if her blood sugar was not regulated and was contributing to her fluctuations. Her A1C came back at a 6.6. (CS#28) Diabetes most acutely affects the microcirculation of the eyes, feet, heart, and kidneys. This patient’s kidney failure was being complicated by an increased blood sugar. Her sugar was not being metabolized properly therefore causing inflammation at the nephron units. After starting four GBS per day, her glomerular filtration rate tripled, the doctors halted her current dialysis regime, and it is hoped that a transplant is no longer needed. There are approximately five current clients in our study who are not improving. However, we believe that there is non-compliance and the clients are not taking four capsules of GBS per day. Our research indicates that admiration of four Gluco-Beta-Stimulator capsules per day for 6-30 months will regenerate the pancreatic beta cells and improve the metabolic disturbances caused by elevated sugar levels in the blood. Failure to comply with this regiment will not see improvement.
As our study proceeds, we are questioning the appearance of patients having an event that is rootly caused by a disruption in the microcirculation. Such events lead us to question many of the associated diseases of diabetes. Do we have the potential to look at people that have an associated disease of diabetes and repair the underlining sugar problem thus halting the advancement of the associated diseases and diabetes?
References
-
Campbell A. The Diabetes Pandemic. Alternative Therapies. 2011;17:8-9.
-
Murray M. Diabetes mellitus. Natural Medicine Journal. 1998;4:4-20.
-
Morrison MK, Lowe JM, Collins CE. Perceived risk of Type 2 diabetes in Australian women with a recent history of gestational diabetes mellitus. Diabetic Medicine. 2010;27:882-886.
-
Wang KL, Liu CJ, Chao TF, et al. Statins, Risk of Diabetes and Implications on Outcomes in the General Population. Journal of the American College of Cardiology 2012;60:1231-1238.
-
Andersohn F, Schafe R, Suissa S, Garbe E. Long-term use of antidepressants for depressive disorders and the risk of Diabetes Mellitus. American Journal of Psychiatry. 2009;166:591-598.
-
Olivarus NF, Siersma V, Dyring-Anderson B, et al. Patients newly diagnosed with clinical type 2 Diabetes during oral glucocorticoid treatment and observed for 14 years: All-cause mortality and clinical developments. Basic & Clinical Pharmacology & Toxicology. 2010;108:285-288.
-
Nielsen J, Skadhede S, Correll C. Antipsychiotics associated with the development of Type 2 Diabetes in antipsychotic-naïve Schizophrenia patients. Neuropsychopharmacology. 2010;35:1997-2004.
-
Ravina A, Slezak L, Mirsky N, et al. Reversal of corticosteroid-induced diabetes mellitis with supplemental chromium. Diabetic Medicine. 1999;16:164-167.
-
Russell, S. Dysglycemia. Professional Complementary Health Formulas, Inc. Retrieved at www.professionalformulas.com.
-
DeCava J. Developing Diabetes. Nutrition News and Views. 2000;4:1-10.
-
Ruhl J. How blood sugar works and how it stops working. Blood Sugar 101. http://www.bloodsugar101.com/. Accessed April 2, 2013.
-
Kaczmar T. Herbal support for diabetes management. Clinical Nutrition Insights. 1998;5:1-4.
-
Leach MJ. Gymnema sylvestre for diabetes mellitus: A Systematic Review. The Journal of Alternative and Complementary Medicine. 2007;13:977-983.
-
American Diabetes Association. Annual Report 2011. http://main.diabetes.org/goh/2011-ada-annual-report.pdf. Accessed March 21, 2013.
-
National Diabetes Information Clearinghouse. Diagnosis of Diabetes and Prediabetes. http://diabetes.niddk.nih.gov/dm/pubs/diagnosis/. Published July 2012. Accessed March 21, 2013.
-
Kirpal D. Type I and Type II Diabetes? Amazing 2,000 year-old lost formula can eliminate the need for insulin and drugs. United States Patent Bulletin. 1999; No924512.
-
Dean, W. Metformin: An effective and underappreciates life extension drug. Vitamin Research News. 12:9.
-
Diabetes Drug Advisory Issued. Modern Herbal Medicine. The Doctors’ Prescription for Health Living. 1999;4:12-16.
-
Pepping J. Cinnamon in diabetes mellitus. Alternative Therapies. 2007;64:1033-1035.
-
Head KA. TyperI diabetes: Prevention of the disease and its complications. Townsend Letter. 1998;July:72-84.
-
Shane-McWhorter L. Dietary supplements for diabetes: An evaluation of commonly used products. Diabetes Spectrum. 2009;22:206-213.
-
Fernadez-Mejia C, Vilches-Flores A, Tovar-Palacio A. Biotin Increases Pancreatic Glucokinase expression via soluble guanylate cyclase/ protein kinase G and autocrine feedback action of insulin. Diabetes 2007;56:443.
-
Bone K. Gymnema: A key herb in the management of diabetes. Townsend Letter. 2002;July:28-30.
-
Kumar SN, Mani UV, Mani I. An open label study on the supplementation of Gymnema sylvestre in type 2 diabetics. Journal of Dietary Supplements. 2010;7:273-283.
-
Ulbricht C, Abrams TR, Basch E, et al. An evidence-based systematic review of Gymnems by the natural standard research collaboration. Journal of Dietary Supplements. 2011;8:311-320.
-
Eiceman G, Hassel E, Nutrition Works, 543 West Franklin Street, Womelsdorf, PA 610.589.5182. Case Study#16. 2013
-
Eiceman G, Hassel E, Nutrition Works, 543 West Franklin Street, Womelsdorf, PA 610.589.5182. Case Study#18. 2013
-
Eiceman G, Hassel E, Nutrition Works, 543 West Franklin Street, Womelsdorf, PA 610.589.5182. Case Study#28. 2013
Share this post
0 comment